A follow-up study on keratopathy in eyes after radiation the
作者 :Qing-Ping Zhang, Chang-Hua Ye, Guang-Wu Huang, Cheng-Xi Xie, Wei-Wei Zhou1, Lin Ruan
【摘要】 AIM: To investigate the ocular complication after radiation therapy for nasopharyngeal carcinoma(NPC). METHODS: The authors performed a previous study on keratopathy in 213 NPC patients who received first stage radiation and had at least 10 months of follow-up. These patients were categorized into three groups depending on NPC clinic stages. Rates and proportions of keratopathy occurring in these groups were compared and analyzed with Chi-square Test and Spearman rank correlation coefficient. RESULTS: Radiation keratopathy developed in 19 patients, about 8.9% (19/213). The latency value was 3 to 30 days. The effect of NPC clinic stages and radiation did on the development of keratopathy was not statistically significant (P>0.05).CONCLUSION: The NPC clinic stages and radiation doses plays few effects on the development of keratopathy. It may play a key role that corneal nerves damage induced ocular surface diseases. It can not be excluded that individuals have different sensitivities to radiation.
【关键词】 keratopathy; ocular surface disease radiation therapy nasopharyngeal carcinoma
INTRODUCTION
Nasopharyngeal carcinoma (NPC) is a most common malignant tumor in Southern China, such as, Guangdong, Guangxi Region, et al.[1] Radiation therapy is still the standard curative treatment in NPC patients. With the development of radiotherapy techniques, the 5-year survival rate of NPC patients was more than 50%[2]. With the delayed survival, the complications induced by radiation become more manifest. However, only the long-term survival rate, the local control, the migration and the radiation damage to brain and spinal cord are more stressed on. There are few studies on ocular injuries in NPC patients who received radiotherapy at present. Tow hundrad and thirteen NPC patients who received first-stage radiotherapy were followed-up. The report is as follows.
PATIENTS AND METHODS
Patients Two hundrad and thirteen NPC patients including 164 male and 49 female patients in this study were received first-stage radiotherapy in our hospital between December 1995 and October 2000. The mean age was 45 years (ranged from 21 to 67 years; standard deviation, 11.3). Pathologically, there were 210 patients with under-differentiated squamous cell carcinoma and 3 patients with alveolate nuclear cell carcinoma. Depended on TNM (the Sixth National NPC Meeting in 1992), they were divided into I, II, III and IV stages with the number of 15, 60, 87 and 51, respectively. Patients were excluded from this study if they had ocular surface diseases or visual path way diseases before radiotherapy.
Methods
Ocular examination The eye and its adnexa were examined in accordance with a standard protocol at head, during and after radiation therapy, including visual acuity, cornea and fundus. The cornea was evaluated using slit-lamp biomicroscopy, including fluorescein staining. Central corneal sensitivity was measured with a Cochet and Bonnet esthesiometer (Luneau Ophthalmologie, Paris, France).
Radiation therapy Radiation of 58 to 82Gy in 1.8- to 2.0-Gy dose fractions was delivered to the tumor 5 to 6 times a week in accordance with the treatment protocol [3]. External radiation with high-energy photon beams of 10MeV was used.
Postradiation follow-up All patient were routinely referred to the ophthalmology department of the same hospital for assessment every three months during the first postradiation year, every six months and twelve months during the second and the third postradiation year, respectively. The mean follow-up value was 15.5?.1months (ranged from 10 to 20 months). Changes in the cornea were evaluated with slit-lamp biomicroscopy, including fluorescein staining every week until patients discharged from hospital. After discharged from hospital, the cornea was evaluated every month during the first three months and every three months after that. Those patients with corneal epithelium damage were treated with antibiotic eye drop and ophthalmic ointment.
Statistical Analysis Data were computed with version 10.0 SPSS. Analysis was done with Chi-square Test and Spearman rank correlation coefficient.
RESULTS
Incidence of Keratopathy There were 231 NPC patients in this study who received first-stage radiotherapy. There were 164 male and 49 female patients, male : female =3.4:1. The mean age was 45 years (ranged from 21 to 67 years; standard deviation, 11.3). Nineteen of them developed keratopathy, about 8.9%(19/213). Of these 19 cases (19 eyes), 12 male and 7 female patients, mean age was 44.7 years (ranged from 29 to 63 years; standard deviation, 8.7).
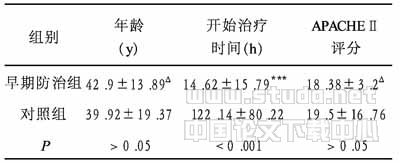
Keratopathy and NPC Stages Keratopathy developed in six eyes in stage I-II (8.0%, 6 of 75 eyes), eight eyes in stage III (9.2%, 8 of 87 eyes ), and five eyes in stage IV (9.8%, 5 of 51 eyes ). Analysis was done with Chi-square Test, which showed no statistical significance between incidence of keratopahty and NPC stages ( P >0.05,Table 1 ).
Keratopathy and Radiation Dose The primary tumor location of NPC patients were received 58 to 82 Gy radiation. Nineteen of patients with NPC developed keratopathy. The influence of radiation dose and developed keratopathy was evaluated by Spearman rank correlation coefficient, which showed no statistical significance between incidence of keratopathy and NPC radiation dose (r's=0.2140, P >0.05, Table 2 ).
Keratopathy and Its Latency Keratopathy occurred in 19 patients during the course of radiation treatment for NPC. They felt dry eye and uncomfortable with no pain, on photophobia and no tearing. Only conjunctive congestion was observed. The latency value of developing corneal epithelium damage was 3 to 30 days. Ten of nineteen patients had keratopathy in 20 days postradiation. The damage of corneal epithelium was slight and the Palisades of Vogt (POV) could still be observed. After 3 to 4 months, the keratopathy healed and visual acuity recovered, however, the corneal sensation was not as fine as the normal. Twenty months after radiation therapy, the corneal sensation still didn't recover to normal. One patient with NPC stage II developed severe keratopathy after 28 days of radiation therapy. Most of POV disappeared. One hundred and fifty-nine days after radiation therapy, there were notable cornea edema and thinning, widespread neovasculization and sensation disappearance. The visual acuity was counting figure /40cm. After radiation 20 months, some new vasculars and most of POV were observed in the cornea. The visual acuity recovered to 0.3. However, the corneal sensation still did not recover to normal. All 19 NPC patients with keratopathy did not developed cataract.
DISCUSSION
As one of the refraction system, cornea plays a key role on maintaining normal visual function. Its constructions are fine. Radiation can induce cranial nerve damage. One or more cranial nerves become paralysis. Hypoglossal nerve is the most commonly seen, followed by glossopharyngeal nerve, abducent nerve and trigeminal nerve.[2] The corneal sensation supplied by the first ramus of trigeminal nerve, plays a key role in the mechanism of cornea protection. The stable relationship between corneal epithelium and tear-film is one of the most important factors to maintain cornea healthy. For maintaining the normal physiological functions of tear-film, the first ramus of trigeminal nerve and the facial nerve, besides the components and hydrodynamics of tear-film should be normal. Winking is a necessary factor to diffuse tear-film. Fujishima et al. [4] found that during infrared radiation treatment, unstable tear-film resulted in corneal temperature changes and winking decrease, which induced corneal epithelium damage. It may explain why corneal sensation disappearance is often correlated with the keratopathy in dry eye. Hallaban et al. [5] found that some genes such as Egr-l, C-jun and NF-kB, began to express after radiation several minutes to one hour. C-jun is one of the protooncogenes. Keratopathy occurred in 19 patients during the course of radiation treatment for NPC. They felt dry eye and uncomfortable with no pain, no photophobia and no tearing. Only conjunctiva congestion was observed. It is possible that radiation damages the corneal nerves and induces ocular surface diseases. So we thought that those NPC patients who received radiation therapy should have ophthalmic examination to diagnose and receive treatment in time to prevent from severe keratopathy, when conjunctiva congestion and/or dry eye are present.
Superficial keratitis, stromal clouding, cell infiltration and edema of the cornea can be observed in radiation keratopathy[6]. Studies showed that after rabbit corneal epithelium damage, if half corneal limbus was protected, conjunctivalisation occurred slightly in a part of the cornea and only a few neovasculars were observed[7]. These neovasculars would disappear in the end. Dua [8] thought that corneal neovascularization was related with the responses of keratitis, hypoxia and corneal stem cell dysfunction. Dysfunction of corneal stem cell might result from nervous keratoapthy and radiation. Our data showed that keratopathy induced by radiation would recover if POV did not lost totally. Clinically, the POV should be evaluated when corneal epithelium injured. Patients should be received treatment in time to prevent from severe complications. Ophthalmologists should have a new concept that dysfunction of stem cell is one of the important links in ocular surface diseases and that stable tear-film and normal corneal construction play a key role in maintaining stem cell differentiation to corneal epithelium.
Zhang et al. [9] showed that corneal nerves could not recover to their normal density and function after they had injured totally 6 months. Fujishima et al. [10] observed one patient with advanced maxillary cancer of left parasinus who received radiation treatment and developed keratopathy. The corneal abnormalities resolved after 4 months with improved visual acuity, but the corneal sensation did not recover to normal at 1year after radiation. In our study, the corneal sensation of the 19 patients with keratopathy did not recover to normal at 20 months after radiation. It showed that repairing and regeneration of the cornea from radiation injury is very slowly. At the same time, we found that the sooner the keratopathy occurred, the slightlier the corneal epithelium damaged and the faster the keratopathy recovered and vice versa, the later the keratopathy occurred, the more serious the corneal epithelium damaged and the keratoapthy recovered slowly. The reason is to be studied.
Radiation damage to human tissue and organ is very complicated. There are secondary responses, besides primary reaction. Different tissues and organs have various tolerances to radiation. The tolerance limit is 6 000 cGY in cornea and 1 200 cGY in lens [1], namely, the tolerance limit of lens is one fifth of the cornea. Various sensitivity of cell correlates not only with the DNA damage, but also with the cell responses to radiation damage[11]. In our study, the 19 patients with keratopathy did not developed cataract at 20 months after radiation. It showed that there was no relationship between cornea damage and radiation dose (r's=0.2140, P >0.05). It possibly correlated with individual sensitivities to radiation.
Keratopathy induced by radiation therapy for NPC is commonly seen and serious damage to visual function may occur. This study showed that keratopathy induced by radiation therapy for NPC possibly related with radiation damage to corneal nerves and ocular surface diseases developing. And it could not be excluded that individuals had different sensitivities to radiation. The authors advise that during radiation therapy, the NPC patients should be treated with antibiotic eye drop and ophthalmic ointment routinely. To prevent from serious damage to visual function, they should visit the ophthalmologist as soon as ocular congestion or dry eye occurs.
【】
1 Gu XZ, Ying WB, Liu TF. Radiotherapy Oncology. Beijing : Beijing Medical University, Chinese Union Medical College United Press, 1993:250,443
2 Kong L, Zhang YW. Late complication of nervous system following postirradiation for nasopharyngeal carcinoma. Chin J Radiat Oncol , 1999;8(3):181
3 Chinese Tumorous Office for Prevent and Cure, Chinese anticancer association coauthor.Chinese common malignant tumour make a diagnosis and give treatment standard -Fifth volume- nasopharyngeal carcinoma. Beijing : Chinese Medical University, Chinese Union Medical College United Press, 1990:21-28
4 Fujishima H, Toda I, Yamada M, Sato N, Tsubota K. Corneal temperature in patients with dry eye evaluated by infrared radiation thermometry. Br J Ophthalmol, 1996;80:29
5 Hallaban D. Radiation-mediated gene expression in the pathogenesis of the clinical radiation response. Semin Radiat Oncol ,1996;6:250
6 Scheie HG, Dennis RH, Ripple RC. The effect of low voltage roentgen rays on the normal and vascularized cornea of the rabbit. Am J Ophthalmol ,1950;33:549
7 Zhao DQ, Sun BJ, Huang AG, He Z, Zheng M, Li JX, Jing WM. Experimental study on the role of stem cells in the corneal limbus of rabbit eyes during corneal epithelial wound healing. Ophthalmic Res ,1996;14(3):149
8 Dua HS. Stem cell of the ocular surface: scientific principles and clinical application. Br J Ophthalmol ,1995;79:968
9 Zhang ZQ, Xie LX, Dong XG. Morphological and functional studies on nerve regeneration after corneal nerve injuries. Chin J Ophthalmol ,1994;30(4):301
10 Fujishima H, Shimazaki J, Tsubota K. Temporary corneal stem cell dysfunction after radiation therapy. Br J Ophthalmol ,1996;80:911
11 Haimovitz-Friedman A, Kolesnick RN, Fuks Z. Modulation of the apoptotic response:potential for improving the outcome in clinical radiotherapy. Semin Radiat Oncol, 1996;6:273